This estradiol patch dosage chart is meant to help you understand what your prescriber is talking about and prepare better questions for your next appointment, not to replace their guidance. Estradiol patch dosing is individualized, based on your symptoms, health history, and how your body responds, and only a prescriber managing your care should make actual dosing decisions or changes.
With that said, here’s how the available strengths break down, how the scheduling works, and the details that are genuinely useful to understand before or during hormone therapy.
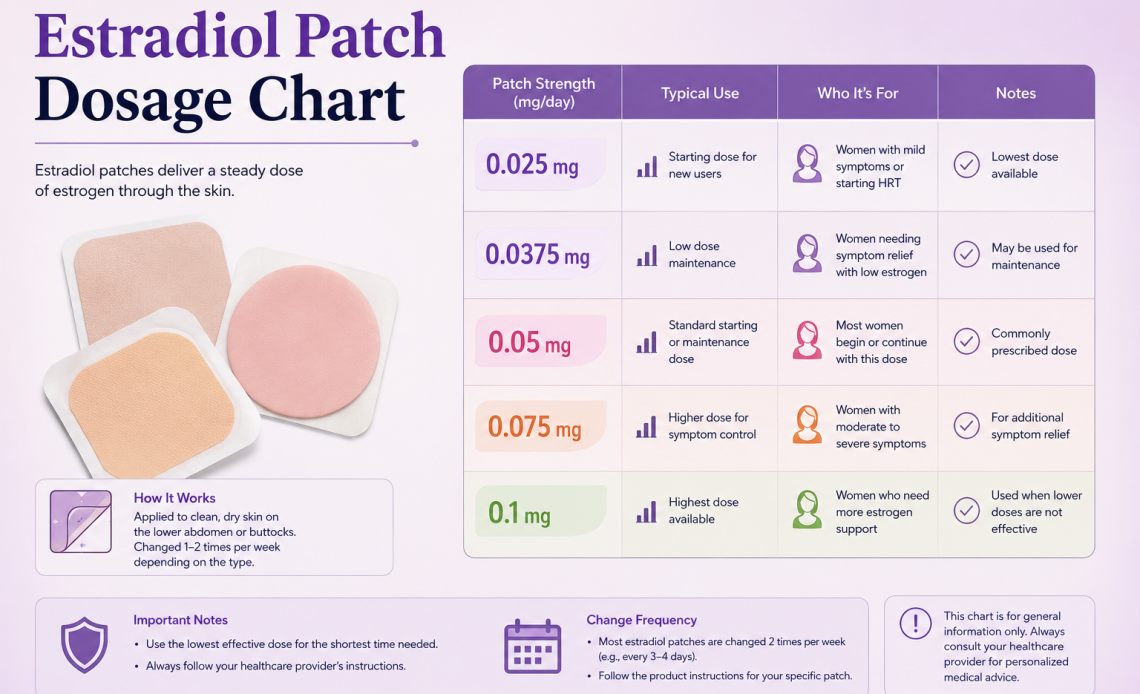
FDA-Approved Strengths at a Glance
| Strength | Typical Use | Common Brand Examples |
| 0.025 mg/day | Common starting dose, especially for osteoporosis prevention | Climara, Vivelle-Dot, generics |
| 0.0375 mg/day | Common starting dose for symptom management | Vivelle-Dot, generics |
| 0.05 mg/day | Standard maintenance dose for most menopausal symptoms | Climara, Vivelle-Dot, Estraderm, generics |
| 0.06 mg/day | Less commonly prescribed intermediate strength | Climara |
| 0.075 mg/day | Higher maintenance dose for persistent symptoms | Vivelle-Dot, Climara, generics |
| 0.1 mg/day | FDA-approved maximum standard strength | Climara, Vivelle-Dot, generics |
Why the Numbers on the Box Aren’t the Whole Patch
Patches are labeled by delivery rate, the amount absorbed per day, not by total drug content. A patch labeled 0.05 mg/day might actually contain anywhere from roughly 0.4 to 4 mg of total estradiol, released gradually over its wear time. This is why patches can’t be cut in half to get a custom dose, doing so disrupts the release mechanism and delivery rate the patch was engineered around, rather than simply halving the dose.
Twice-Weekly vs Once-Weekly Patches
| Twice-Weekly (e.g., Vivelle-Dot) | Once-Weekly (e.g., Climara) |
| Changed every 3 to 4 days | Changed every 7 days |
| Smaller patch size | Larger patch, holds a bigger reservoir |
| Tends to have more consistent adhesion | Adhesion can weaken by day 5 to 7 |
| More frequent site rotation needed | Fewer changes, but larger area affected each time |
How Starting Dose and Adjustments Typically Work
- Most prescribers start at the lowest strength likely to help, often 0.025 or 0.0375 mg/day.
- Response is generally assessed over 4 to 8 weeks before considering an adjustment.
- Dose increases are typically made in the smallest available increment rather than large jumps.
- The general prescribing principle is the lowest effective dose for the shortest duration needed to manage symptoms, reassessed periodically rather than continued indefinitely by default.
- If breakthrough symptoms occur shortly before a scheduled patch change, that timing itself is useful information to share with your prescriber.
The Progesterone Question This Chart Doesn’t Answer Alone
Dosage strength is only part of the picture. If you have a uterus, estrogen therapy is generally paired with a progestogen to protect the uterine lining, since unopposed estrogen use is linked to a higher risk of endometrial cancer. This isn’t something a patch alone addresses, it’s a separate prescribing decision your provider makes alongside the estrogen dose itself. If you’ve had a hysterectomy, this consideration typically doesn’t apply, though some exceptions exist depending on individual history.
A Detail Most Charts Leave Out: Brands Aren’t Perfectly Interchangeable
Two patches labeled with the same delivery rate don’t necessarily produce identical blood estradiol levels, since adhesive formulation affects how efficiently the hormone actually crosses into skin. This is part of why some people notice a difference, breakthrough symptoms or side effects, after switching from a brand-name patch to a generic at the “same” labeled dose. If that happens to you, it’s worth mentioning to your prescriber rather than assuming something else is wrong.
Practical Application Tips
- Apply to a clean, dry area of the lower abdomen or upper buttock, never the breasts
- Avoid the waistline, where clothing friction can loosen the patch
- Rotate sites, waiting at least a week before reusing the same spot
- Press firmly for at least 10 seconds, especially around the edges
- If it lifts, press it back down; if it falls off completely, replace it and continue the same schedule
- Swimming, bathing, or sauna use may loosen adhesion, plan patch changes around these activities when possible
What Warrants a Call to Your Provider
- Any new or unusual vaginal bleeding
- Signs of a blood clot: leg swelling, warmth, or pain, sudden shortness of breath, or chest pain
- Sudden severe headache, vision changes, or one-sided weakness
- Persistent breast pain or a new breast lump
- Skin irritation at the application site that doesn’t improve with site rotation
Most side effects reported in clinical trials, like mild breast tenderness or headache, are far less urgent than the list above, but the items here specifically warrant prompt medical attention rather than waiting until your next scheduled visit.
Hormones Affect More of the Body Than People Expect
Estradiol dosing gets a lot of attention because of its role in menopause management, but it’s a good reminder that hormonal fluctuations generally, not just estrogen replacement specifically, can affect symptoms well beyond hot flashes, including digestion, mood, and energy.
If you’re navigating hormone-related symptoms more broadly, our piece on whether it’s normal to have diarrhea on your period covers another common way hormonal shifts show up in the body, and when digestive symptoms tied to your cycle are worth mentioning to a doctor.
A Couple of Things Worth Correcting
Cutting a patch in half doesn’t give you half the dose reliably. It disrupts the engineered release mechanism and can result in unpredictable, inconsistent absorption.
A higher dose isn’t automatically more effective for symptom relief. Current prescribing guidance favors the lowest effective dose, since higher doses increase certain risks without necessarily improving symptom control beyond a certain point.
Switching brands at the “same” dose isn’t guaranteed to feel identical. As covered above, differences in adhesive formulation can meaningfully change how much estradiol actually reaches your bloodstream.
Bottom Line
Estradiol patches are available in six standard FDA-approved strengths, from 0.025 to 0.1 mg/day, with most people starting low and adjusting based on symptom response over several weeks. The delivery rate on the box isn’t the total drug content, brands aren’t perfectly interchangeable at the same nominal dose, and anyone with a uterus needs a progestogen alongside estrogen therapy. Use a chart like this to understand the landscape and ask better questions, not to make dosing decisions independent of the provider managing your care.
Common Questions About Estradiol Patch Dosing
What is the most commonly prescribed estradiol patch dose?
0.05 mg/day is generally considered the standard maintenance dose for most menopausal symptom management, though starting doses are often lower.
Can I cut my estradiol patch to adjust the dose?
This isn’t recommended without specific guidance from your prescriber, since it can disrupt the patch’s designed release rate and lead to unpredictable absorption.
How long does it take to feel the effects of a dose change?
Most prescribers assess response over 4 to 8 weeks before making further adjustments, since it takes time for symptoms to reflect a new steady-state hormone level.
Do I need progesterone with an estradiol patch?
If you have a uterus, yes, typically, to protect against endometrial cancer risk from unopposed estrogen. This is a separate prescribing decision from the patch dose itself.
Is a higher mg/day patch always better for symptom control?
Not necessarily. Guidance favors using the lowest effective dose, since higher doses increase certain risks without guaranteed additional symptom benefit.
Can switching from a brand-name to a generic patch change how I feel?
It’s possible, since different adhesive formulations can affect absorption even at the same labeled dose. Mention any new symptoms after a switch to your provider.
What should I do if my patch falls off before the scheduled change day?
Reapply it if possible, or apply a new patch to a different site and continue your original schedule from there, rather than restarting the full interval.
Who should not use an estradiol patch at all?
People with a history of certain blood clots, stroke, heart attack, or certain hormone-sensitive cancers are generally not candidates, among other contraindications a prescriber will screen for before starting therapy.